

Editor’s Note: This story is the first part of a two-part series on 988. This piece addresses the increase in unwanted or coercive police interventions after 988’s implementation. The second part addresses issues around privacy and the sharing of the contents of conversations for AI development.
Two years and a billion dollars in, the 988 Suicide and Crisis Lifeline continues evolving rapidly. Vibrant Emotional Health (Vibrant), administrators of 988Lifeline under contract from the Substance Abuse and Mental Health Services Administration (SAMHSA), has spawned a political lobbying division that’s helping usher state infrastructure investments and legislative initiatives. The developments are aimed at gradually reshaping a loose network of call centers into a coordinated access hub for America’s “crisis care continuum” and mental health service system.
However, none of this is stemming the stream of 988 callers who receive unasked for, unwanted, or unexpected visits from police and emergency medical services (EMS)—and then get taken, with or without consent, to hospitals or crisis centers for mental health evaluations. Some report having been further subjected to forced stripping, solitary confinement, prolonged detentions, and even involuntary treatments.
Callers to 988 targeted by these practices describe feeling misled, betrayed, and ultimately battered by their experiences. And, contrary to 988 promoters’ promises of “getting police out of crisis care” and previous public assurances from SAMHSA and Vibrant about the low frequency of these police/EMS interventions, stunning new data show that the intervention rates have in fact skyrocketed—quadrupling in 988’s first year. And rates of police/EMS interventions on callers who discuss suicidal feelings appear to be even higher.
Openness is risky
A California-based mental health advocate and speaker, last summer Emily Wu Truong was distraught near the anniversary of her father’s death. She was out walking late at night, and didn’t want to bother relatives or friends, so she called 988.

Truong said she was not actively suicidal, but called so she could confidentially open up about her sadness and suicidal feelings—what 988Lifeline ads say the service is for. “I wanted to be anonymous while processing my emotions,” she said.
Truong did not know, and her local call center’s website did not disclose, that 988Lifeline’s “imminent risk” policy requires call-attendants to potentially contact 911 to trace calls and send out police/EMS if a caller expresses “a desire and intent to die and has the capability of carrying through.” NextGen911 allows tracking mobile devices to within three yards and, typically, police/EMS then take these callers—with or without consent—to a hospital or crisis center for psychiatric evaluation. Some call centers have started disclosing this practice, but often still mislead users; for example, SAMHSA’s 988 website says that call-attendants contact 911 only when there is “an immediate risk to life”—yet the actual policy explicitly states that it should be applied far more broadly.
The goal is to stop callers from killing themselves. But studies show that, for every person who’ll actually kill themselves, hundreds of others have desires and plans. Even experts barely beat random chance in predicting suicides.
People like Truong can get ensnared. In conversation, her emotions are close to the surface, and frequently flow out as expressively as the colorful outfits she often dons. It’s easy to laugh along with her exuberance—and tear up or fret about her sorrow. “I’m very public about my emotions and expressions,” Truong acknowledged. “So [the 988 call-attendant and first responders] were probably overwhelmed and at a loss. They didn’t know how to handle my over-expression. I was crying a lot, too.”
While pouring her feelings out to the 988 call-attendant—including without filter mentioning exactly where she was—paramedics arrived. Truong was taken to a noisy emergency room, forced into scrubs, monitored in the bathroom, put in solitary confinement, restrained in a gurney for transfer, and then detained in a psychiatric hospital. The experience, she said, felt like she wasn’t in a helping setting but “in a jail.” She was offered drugs but no therapy, and after two days of stress wondering why she couldn’t leave, she was sent home with $4,500 in medical bills.
“How does this promote healing?” Truong said, furious that a few people “overreacting” to her open emotions led to her psychiatric incarceration. “It’s traumatizing. It’s a living nightmare.”
When she asked for the recording of her call to buttress her complaints to 988Lifeline, Vibrant told her she’d have to get a court order—a policy Vibrant has implemented.
“If you want people to trust you, you need to show transparency,” said Truong. “Where’s the accountability?”
Elle has the same question—she felt threatened by the call-attendant and also got detained, and Vibrant refused to release the recording of her call as well.
Go to a hospital—or else
Elle (not her real name), a law student in her early 20s, often experiences traumatic flashbacks from a history of sexual assaults. A therapist recommended 988.
Last autumn, Elle called. “I just wanted somebody to walk me through those flashbacks and do things like grounding techniques or breathing exercises,” she said. “It’s just really nice to have another person as an anchor.”
Elle found the 988 call-attendant helpful. After ten minutes, though, the call-attendant asked her what city she was in, then abruptly transferred her call to that city.
The new call-attendant immediately pressured Elle for her full name and address—repeatedly. “Given the nature of my history, which involves stalking and assault, I was very, very uncomfortable giving her this information,” said Elle.
The call-attendant also asked Elle if she was suicidal—repeatedly. “I wasn’t suicidal. But I might have said something like, ‘I want all of this to stop.’ Meaning, my flashbacks. I was having severe flashbacks throughout this.”
The call-attendant asked if she was going to kill herself how would she do it. “She just kept pressing this issue of suicidality,” said Elle, who was not told she was being put through 988Lifeline’s risk-assessment. “I felt like I needed to answer. I felt like I couldn’t hang up. In the situations that I have been in with predators, I often found that the path of least resistance was the path that led to the least pain; so, you do what they want.”
Elle suggested she might jump from a nearby high-rise or obtain pills. The call-attendant then insisted that Elle drive to a psychiatric facility. Elle declined. “She told me that if I did not come in, she would have to send the police to my house.”
Elle drove herself. “I very much did not want the police to come and drag me out of my apartment.”
At the psychiatric facility, staff took away Elle’s belongings, including her smartphone and, over Elle’s pleas, a bracelet she’d worn every day since her late-grandmother gifted it.
Elle had never experienced psychiatric incarceration. “I didn’t know what was happening,” she said. “I was very terrified… Every access I had to the world was taken away from me. I could not keep the small things that might have brought me comfort.” She was confined in a room about six feet by nine with three chairs and a blacked-out window. She knew from her law studies that seclusion is extremely dangerous for prisoners—but never imagined she’d experience it herself. She pulled two stiff chairs together and curled up across them, hugging herself for warmth.
Hours later, two men strapped her to a gurney and drove her to a psychiatric hospital. After hours more waiting alone, Elle was ordered to sign intake forms.
“One of the forms was whether I was allowing myself to be admitted voluntarily or whether it was an involuntary admission.” Elle asked, if this was a voluntary admission, then could she leave? The admissions coordinator told Elle that if she didn’t sign in voluntarily, the detention would last much longer. By this point, Elle said her flashbacks had retreated and her “lawyer mind” was “kicking in.” She stifled an impulse to reply, “Fuck you, you goddamn bitch.” Later, Elle would study her state’s commitment law and submit complaints about the institution’s processes.
Over the next four days, Elle and others were corralled into a common room by day, where male patients frequently sexually harassed the younger women. One man talked about clothing he wanted to see Elle wearing, put objects she touched in his pants pockets, and described wanting to track her down outside hospital. By night, with no lock on her room’s door, Elle didn’t sleep.
“I wasn’t suicidal going in, but I sure was coming out,” said Elle.
In its April 2024 Report to Congress, SAMHSA admits “no research” validates 988Lifeline’s emergency intervention policy—while some research suggests psychiatric hospitalization may well heighten suicidality. Elle has frequent nightmares about the hospital, and scans streets for the threatening male patient to “make good on his promises.”
For Elle, involuntary psychiatric detention “was like being assaulted again, but in your entire brain, and also your soul.” With disturbing, visceral imagery, Elle described her experiences of sexual assault as being treated like an animal “valued” only for its “meat.” But in the psychiatric hospital, she said, “It’s like I was a rat, or a gnat… I don’t think it mattered to them whether I lived or died, beyond their own legal liability.”
After learning more about 988Lifeline’s intervention practices, Elle said, “It’s really frightening and inappropriate that somebody can ruin your life based on a ten-minute phone call.”
Vibrant and SAMHSA have long publicly said less than 2% of 988 calls lead to such police/EMS interventions and hospital detentions—but haven’t released actual data. Through a freedom of information request, Mad in America confirmed this rate from a 2017-18 national survey of crisis call centers.
Vibrant has also claimed that many emergency interventions occur “with consent” of callers, but former call-center staff challenge such characterizations. Notably, since Elle drove herself to hospital and Truong disclosed her location, both interventions would apparently be listed as “with consent.”
Recent data from one major 988 call center shed light on exactly how, and how often such interventions truly occur.
Types of intervention, levels of coercion
The New Mexico Crisis and Access Line (NMCAL) is operated by Protocall, a company that also runs hotlines for schools, communities, and corporations.
Wendy Linebrink-Allison, Protocall’s New Mexico Program Manager, said that their 988 contract with the state mandates aggregated public reports. Protocall supports the practice for providing insights about who’s calling and why. “It has really benefited our community partners,” said Linebrink-Allison. “They’ve always expressed appreciation.”
Linebrink-Allison understands criticisms of unwanted interventions by people like Elle and Truong. “I want to encourage people to continue to share their voices to facilitate change,” she said. But she worries negative stories can make people wary of calling. “I don’t want, at any point, people to feel like there’s no place for them to call.”
The data alone might make some feel that way.
Many 988 call centers, including NMCAL, still also take calls through a local 800-number crisis line, and combine data. Overall, police/EMS interventions occurred on 3.5% of all calls to NMCAL. (In most of the data discussed in this story, “contacts” or “calls” to 988 through text, chat, and phone are combined.)
However, the majority of calls to NMCAL don’t involve people discussing troubles. Protocall defines “clinical calls” as those involving someone discussing a serious concern instead of, say, just seeking information. According to their year-end report, clinical calls composed about 40% of their crisis line contacts in 2023.
For these clinical calls, NMCAL’s data describes interventions such as getting callers to contact 911 themselves, making a conference-call connection involving caller, call-attendant, and 911 dispatcher, and contacting 911 without caller consent.

Linebrink-Allison said these reflect the steps their call-attendants take. “We want to make sure that we’re involving people in their decisions, and we’re allowing people choice and a voice… We don’t threaten people… We encourage people to engage in what is best for them.”
Still, on average in 2023, at least 6.3% of clinical calls led to interventions apparently involving pressure or coercion, with 911 or police contacted by call-attendants rather than by callers.
Furthermore, only 27% of clinical calls involved people talking primarily about suicidal feelings, as opposed to work stresses, anxiety, substance abuse, or other concerns. People with suicidal feelings were targeted for coercive interventions much more frequently—in 15.1% of cases.
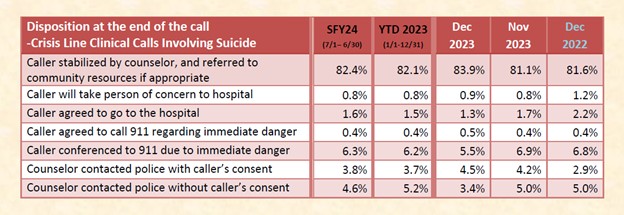
In other words, people primarily discussing suicidal feelings had odds of nearly one in six of getting an unwanted visit from police/EMS.
These rates seem high compared to SAMHSA and Vibrant’s claims—however, stunning new national data shows NMCAL implements such interventions less frequently than average.
Skyrocketing rates of interventions
A recently-released national survey conducted by NRI, the research arm of the National Association of State Mental Health Program Directors, gathered data on 3.5 million calls in 2022—about half to 988 call centers and half to non-988 centers (including centers that answer both 988 and local 800-lines). The survey found that, of all contacts, 3.6% resulted in law enforcement being dispatched, 1.9% resulted in EMS dispatch, and a further 2.3% of calls were transferred to 911 “which may have then dispatched law enforcement or EMS.”
In total, then, 7.8% of all contacts of all types received police/EMS interventions—nearly four times the rate previously claimed by Vibrant and SAMHSA.
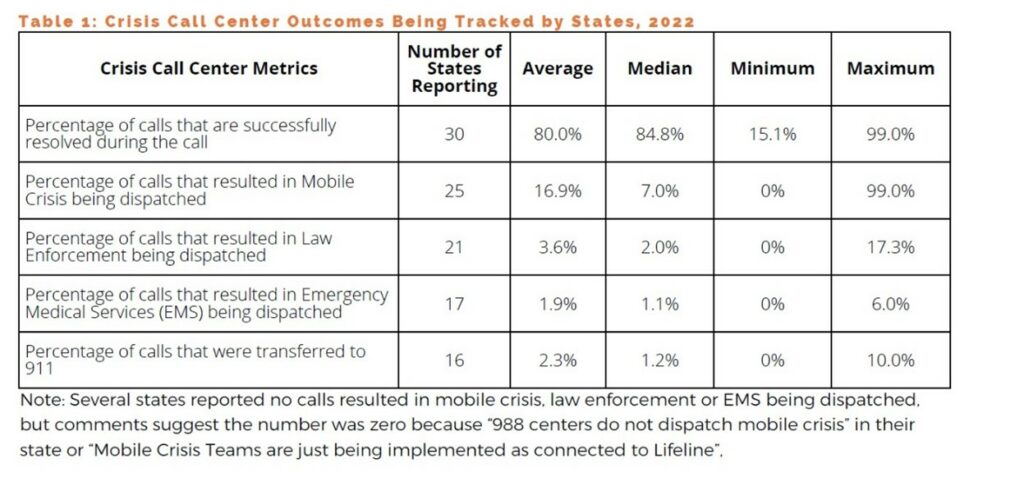
What’s also striking are the wide variabilities; in one state, over 17% of all callers got police visits, and in many others, below 2%.
How many people does this represent? During that first year following the launch of 988 in 2022, the 988Lifeline handled about 5.2 million contacts. So, more than 400,000 callers that year received visits from police/EMS, and were likely taken to psychiatric institutions.
Mobile crisis teams (MCTs) are touted as a less-coercive alternative. But according to the same survey, 16.9% of calls resulted in MCTs being dispatched—and MCTs got hundreds of thousands more people taken to hospital emergency rooms or crisis centers.
When I presented the striking NRI findings to Vibrant and SAMHSA, they declined to comment, and did not provide other data.
Since many non-988 crisis lines implement interventions as well, the total numbers of people around the country affected each year are still higher.
Told of the 988 numbers, Truong cried, “People are just trying to find a helpful listener to validate and hold space! It’s fucking unacceptable.”
“I feel appalled,” said Elle. “Horrified. Angry. It makes you wonder how many of those people will never recover.”
Liz Latty helped research a forthcoming Trans Lifeline report on crisis hotlines, focusing on experiences of users from marginalized communities—including BIPOC, LGBTQ+, and self-identified disabled and mad people. Latty said many described damaging long-term impacts from these unwanted interventions on their privacy, safety, sense of identity, finances, and more. “It devastates people’s lives,” said Latty.
What’s driving it?
Since Vibrant and SAMHSA have for years refused to publicly release data on these interventions, it’s unclear if the rates have risen steadily across the country since 2018, or if the launch of 988 precipitated a sudden, massive increase.
The latter is certainly plausible: Early on, even proponents of 988 worried what might happen with a huge upsurge in calls coupled with no significant increases in mental health supports in communities to direct people to.
There could also be other factors at work.
It would obviously be simple to change the policy to implement interventions only with expressed consent of callers. And indeed, partly due to criticisms of the imminent-risk intervention practices from inside and outside 988Lifeline, during the original drafting of 988 legislation, the federal government declined Vibrant’s requests for direct access to 911’s call-tracing technology. Congress instead ordered a stakeholder consultation. However, the software company RapidDeploy has developed a technical workaround. Already installed by Mental Health America of Greenville County (MHAGC), 988 call-attendants in South Carolina can connect directly to 911’s call-tracing system. RapidDeploy said in 2022 that South Carolina was “the first of many states.” These and other tightening relationships between 988 and 911 could be part of what’s driving the rising rates.
Neither MHAGC nor RapidDeploy responded to requests for interviews. SAMHSA and Vibrant declined to respond to questions about 988Lifeline uses of RapidDeploy.
SAMHSA also hinted to Congress that Vibrant could be using “new technologies” to “enhance the precision of identifying imminent risk situations”—in other words, AI bots may be monitoring calls and flagging people for police/EMS interventions, as occurs in Canada’s 988 system. Such alerts could generate bias or even put pressure on call-attendants.
Even as these questions hang in the air, though, SAMHSA’s obscure remarks to Congress about new technologies and 988 serve as a cryptic warning about a vast new frontier opening up for entirely different kinds of breaches of confidentiality and privacy. There appears to be a goldrush on among researchers, AI developers, and corporations as Vibrant and 988 call centers have started sharing recordings and transcripts of the intimate voice, chat, and text conversations of people contacting 988.
Thanks for showing people the truth about this, Rob. There was and is so much propaganda about 988. It’s promoted as something new and different, safer, kinder. The message is “we get it”. Clearly they don’t.
I’ve been bombarded recently with ads for the 988 number in my state. The tagline: “It’s okay to not be okay.” Apparently, it’s not okay.
The double speak is dystopian. I’m sorry to everyone who has been harmed by the false sense of safety that 988 messaging creates. I know from personal experience that the trauma of forced “treatment” can last a lifetime.
Report comment
Thank you for your insightful story, Rob. I look forward to reading part two. I have never called a hotline out of fear that it could result in a forced hospitalization. I have had two hospitalizations after attempts in 1994 and 1995 and the takeaway was I never want to have to endure that experience again.
My fear of another hospitalization was so great that I did not discuss my ongoing intermittent ideation in therapy until 16 years later. I have learned to frame my symptom as passive to therapists and prescribing professionals to prevent unnecessary intervention. I have found that talking about it has helped diminish the intensity. Suffering in silence is less safe for me. I have a few close friends that will hold space for me and this has been a key tool in managing my ideation for years.
In my advocacy public speaking and writing of my experience, I haven’t promoted 988. Your article has validated that my fear is not unfounded, and to continue educating people on how to hold space for one another. Thank you, again.
Report comment
Thanks for sharing your perspectives, Marianne. I agree–honest, open, safe, confidential connecting with others is such a vital part of being human. And it disturbs me to no end that 988 is advertising that promise and then pulling the floor out from under people.
Report comment
For all practical purposes, it’s become illegal to express sorrow and hopelessness.
We live in a fucked-up world.
Report comment
Yes, we do, Birdsong. It’s getting more so by the day.
Is anyone to believe that this is anything other than the 988 system fulfilling it’s true purpose, I wonder.
Report comment
I wonder too. Calling the cops on desperate people makes no sense whatsoever.
Report comment
Thank you both for your support and encouragement. And I share your question! From 988 administrators I often hear a sense that they believe they are literally “saving” so many lives, and therefore destroying some other lives along the way isn’t such an important thing on balance. But I haven’t seen much evidence to support that view, and I start to wonder why they apparently believe it so strongly.
Report comment
I’d guess so they can avoid the horrendous cognitive dissonance one must feel from ‘helping’ people by imprisoning and tormenting them. I would give most the benefit of the doubt and say they probably got into that line of work with a genuine desire to help, but maybe I’m naive.
Report comment
I’ve quoted this elsewhere but repost here because I believe it relates to your question Mr Wipond.
“The welfare of the people in particular has always been the alibi of tyrants, and it provides the further advantage of giving the servants of tyranny a good conscience.”
― Albert Camus
I do believe that these people are gradually losing their minds, thinking that it’s just a matter of earlier and earlier interventions. And once caught on that Hamster Wheel it’s nigh on impossible to get off.
It’s about to get interesting where I live. As a result of a shooting the premier wishes to make it mandatory for ‘medical staff’ to report suspected potential violence to Police….. and ‘interventions’ will follow. Precrime, despite the ‘medical staff’ pointing out the fact they’re no better than anyone else at predicting the future…. but they have been misleading the public about their ‘magic powers’ …. our Chief Psychiatrist accepting that a nurse can read minds and travel trough time and space.
Who would have thought the State would be providing a means to destroy peoples lives with a phone call? Hello? Einsattsgruppen? I’ve got a suspected Jew living next door to me……
https://www.youtube.com/watch?v=oZ9UQKBUrsg&t=2s
And there are some “concerning aspects” to this ‘help’ being provided to this man….. concerning that the media published it before the State could cover it all up. Though I do note the man was placed in an induced coma while they “edited” the legal narrative.
Look forward to reading part 2.
Report comment
I would have to wonder if the more people that are referred (coerced), equals more funding for call centers.
Report comment
DUH! OF COURSE it’s all about $$$$….and power & control…..lol
It’s what the Social Justice Warriors of the Democrat Party **DO***, it’s WHO THEY ARE….Raise taxes, bigger Government, more $$$ & power for them….
Report comment
Hi Bill, just want to tell you how much I feel for you. The swat scenario you describe brought back visceral memories from 17 years ago. It wasn’t political, it was a Mica Miller scheme to steal an inheritance – I felt like I was being forced into diagnosis. I was blacklisted from my career, across states as I tried to distance myself from the family but one thing I want to tell you – it’s not a red/blue thing, it’s about the green.
My sincere condolences for your experience of torture and injustice. There but for the grace go we all.
Report comment
Third party calls resulting in involuntary detentions need to be closely scrutinized and legal support for targets needs to exist – in California false imprisonment via 988/911 is only a 6,000 $ fine while the record and reputation of the target is destroyed.
Report comment
Services like this are not a safe option under any circumstances.
Report comment
How does further trauma make someone want to live???
Report comment
When did being at your wits end become a crime???
Report comment
I live in Albuquerque and the police came to my door at about 9pm because someone had called NMCAL pretending to be me and said that they were suicidal. I had to deal with an agressive cop who treated me like a liar. I requested to see the information that he was provided and I demanded to hear the call, becuase I know it was not me. I called NMCAL who could see that my number never called. I complained and there was no followup. I wanted them to release the phone number that I allegedly called from and they never did. I would never use this service based simply on my interaction with this police officer trying to get inside of my house and treating me like a criminal.
Report comment
Thanks for putting that out there. SWATting is a crime, making a false report to police. The aggressive police behavior is harassment. Of course the law wants you and your story to go away. I wish I knew a lawyer who would help targets of swatting.
Report comment
Never heard it called that Lucy…. SWATing. I like it.
I know there are legal protections from ‘mental health workers’ in our Criminal Code which carry a 3 year prison term for unlawful procurement of a person…. but its window dressing. In all the years it has existed there have been 2 charges laid, and zero convictions…. so it’s a license to kidnap if your an Authorised Mental Health Practitioner.
Add to this that with the LIE the AMHP tell to police (claiming a citizen as their “Outpatient”), they can induce an “acute stress reaction”…… and well, in my instance I had been ‘spiked’ with date rape drugs (benzodiazepines) before the acute stress reaction was induced. By having police think they are assisting with an “Outpatient”, the AMHP can create the false belief in his/her collegaues that they were requested to do an assessment for police….. thus fabricating a “referral source”. It’s quite a clever means of committing offences. The AMHP calls police for assistance, has them force the citizen into an interrogation, forge the Forms, and have Police deliver your victim to the hospital where it looks like Police have requested assessment from AMHP ….. the perfect crime.
The two DO NOTs of an “acute stress reaction” are (a) Do Not force the person to talk, and (b) do not administer benzodiazepines. Now I’m going to assume that these ‘professionals’ were aware that this was the case and well, basically they’ve found a method to torture people and not be held to account. It fits the definition in Article 1 of the Convention against the use of Torture (which I know the US has not ratified)
Don’t wish to talk about your problems? Okay, that justifies you being ‘spiked’ with date rape drugs and then have a pistol put to your head to make you talk…… now were getting somewhere with your ‘treatment’ you don’t want or need.
Drugging people without their knowledge is also a crime, and particularly when two people get together and plan to do it in order to commit other serious offences but …. once you’ve enlisted the Police to materially support you in your crimes, well, they’ll look the other way while a doctor ….. some of them do have the stomach for it…..
All very ugly of course and the amount of hypocrites I’ve met as a result. I’m sure they mean well when they boast about how they’re advocates for the mentally ill and ….. will promptly look the other way while the State viciously assaults people for complaining.
Still, the fact is I gained a knowledge of the mental health codes….. a request for an “acute stress reaction” by police is code for torture them because they likely won’t talk. “Regular medications” are what they administer without your knowledge to ‘enhance’ the effects of those “acute stress reactions”, and obtain your ‘compliance’. And I find it fascinating that Australia calls this torture when it’s done in Ghana (see complaints to the UN) but call it ‘we’ll fuking destroy you and your family if you try and complain about us and we’ve got police helping’.
Oh, and “editing” of medical records…….that really concerned me because we have euthanasia laws and if they can “edit” those legal narratives in the same manner, we have a real problem. But like the 988 people, they need to create a false belief that they’re good guys despite the odd ‘unintended negative outcome’ (this being a euphemism which came out of our largest facility when a number of people had their necks broken and died as a result of restraints) I assume the facilites elsewhere employ thugs that like to practice their ‘techniques’ on the ‘patients’?
Report comment
Daniel, that’s a shocking and disturbing story. I agree–you would think they would release the number and the police could prosecute. If you might like to collaborate on trying to delve into this more, drop me an email or contact me through my website.
Report comment
On Sept. 22, 1998, two employees of the local “Community Mental Health Center” called the local police, LIED, and claimed that I was suicidal. The Police used that lie as an excuse to mount an almost-literal POLICE RIOT at my apartment, including an officer with a shotgun pointed at my window standing behind a tree in the yard. I was forced to open my door to keep them from breaking it down. I was dragged in handcuffs to the local hospital ER, where they tried to force me to meet with some “emergency services” worker, and to admit that I was suicidal. I was NOT suicidal, so the cops then took me to the Police Station, arrested me for a specious criminal charge, and held me for $500. CASH BAIL…. 6 months later, at trial, the Police Prosecutor dropped the charges, because they weren’t even legal charges in the first place! Trust me, that’s just the tip of the iceberg of the bad behaviou that is daily inflicted on disabled persons…..
Know any good lawyers licensed in the State of N.H.?….
Yes, I realize that “good lawyers” is most often an oxymoron….
Report comment
Thank you for your dedication and persistence, Rob. I wish there were a way to know how many suicides are directly or indirectly caused by psychiatric interventions, whether these are “voluntary” or involuntary.
Report comment
It’s a tragedy that we have no safe place to go. I have a long history of forced hospitalizations and so now I trust no one. Not my doctor. Not my psychiatrist. Not friends or family. I’m even scared to post this, but I feel it’s important to share this.
Thank you Rob, Birdsong and KateL.
It feels true that mental illness, even just human pain and grief, is now illegal.
Report comment
Melpomene,
I really get that. I also have had many forced hospitalizations, many of which happened in the 5 years or so following ECT. After ECT, when I was suffering from unacknowledged cognitive impairment, I received a borderline personality dx and was put on an ever-changing series of psych drug “cocktails” (always including anti-psychotics). I know now that I was suffering from psych drug induced akathisia, but the symptoms of this condition were always blamed on my “mental illness” and “poor coping skills”.
The forced “interventions” almost always involved police and were both humiliating and traumatic. I felt that the goal was to “teach me a lesson”, not to help me.
I have the same problem now of not being able to trust. People talk about “getting help” and almost never acknowledge that the “help” is often actually just more layers of trauma, leading to hopelessness and isolation.
Report comment
We have a lot in common. My mental and physical collapse happened 30 years ago and I had a very full life as an artist and working wife and mother. I fought hard to get my life back and put myself in the hands of a highly respected psychiatrist at Mass General. I underwent 12 ect treatments, both types – side to side and back to front. This left me with profound memory loss and further loss of my ability to function. In frustration over not being able to express my anger and despair, I became a “cutter”. Bleeding was my way of letting out my pent-up feelings. I was not suicidal and never cut myself so badly it would be life-threatening. That earned me the Borderline Personality diagnosis. And more anger and frustration. Mild depression became severe treatment resistant major depressive disorder. Over the years I accumulated PTSD, General Anxiety disorder, fibromyalgia and several phobias – the most disabling of which keeps me homebound. I blame several of these on my supposed treatment and multiple hospitalizations.
I have lost my mother, two brothers and my husband to suicide. Of COURSE I feel suicidal sometimes, but not actively. I hold it as a future option if things become more unbearable. But do I talk about this? What do you think?! ❤️
Report comment
Melpomene,
It is so devastating to hear what you’ve been through in this system, knowing that experiences like yours and mine are not at all rare. It seems as though our big mistake was ever putting any trust in the system and acknowledging that we were in emotional pain.
I’m so sorry for the losses you’ve experienced, and that it’s still so unsafe for you (and I, and so many others) to express ourselves and the truth of how we feel.
I get comfort from hearing from others who feel the same, but I so wish that we could support each other in “real life”, as they say.
Report comment
These stories break my heart – when it happened to me 2007, it was a smear campaign to steal an inheritance, and I knew it at the time. But I’m still affected in ways that are like being crippled.
I’ve asked Rob about an article exposing the experiences of those who’ve been swatted, detained because of a third party report. He would he said, if he could find people who would go on record. I definitely would, it’s a burning need for me.
Report comment
“BAD HELP IS WORSE THAN NO HELP AT ALL”, has been one of my mottos since I escaped psychiatry and the local “community mental health center” in 1996….
Melpomene, KateL, & Lucy SPEAK TRUTH….
Report comment
I get it, too Melpomene. The fear never completely goes away, and it happened to me only once decades ago. I’ll never understand the rationale behind it.
Report comment
As a mental health consumer with suicidal ideation (currently in treatment) this is especially concerning. If it is further publicized it may actually be a *deterrent* to people calling for support. If they are experiencing ideation but not plans, the possibility of hospitalization (incarceration!) against their will may keep them from accessing necessary support in order to work through their crisis. Thank you for your advocacy on our behalf, and please continue to get the word out. This process needs to be corrected, and quick! Best regards.
Report comment
Thanks Rob for doing such commendable and important investigative work. It’s telling they refuse to release data and don’t respond to requests for interviews etc. Until someone gets ensnared by the hypocrisy of the mental health ‘care’ system they don’t know how much harm they can be subjected to. It can even be a third party with ill intentions that calls these ‘help’ lines to make up fabrications about someone else and cause lasting harms.
Report comment
Thank you, Rob, for your truthful – albeit re: a sad state of affairs – reporting. It’s so frustrating to know the truth about the iatrogenic nature of the so called “serious mental illnesses,” yet those industries only respond by trying to make things worse, due to their desire to “maintain the status quo.” A “status quo” that no sane and decent person should want to maintain.
https://archive.org/details/pedophila-empire-satan-sodomy-the-deep-state-ch-1-25-joachim-hagopian.epub/Pedophila%20%26%20Empire%3B%20Satan%2C%20Sodomy%2C%20%26%20the%20Deep%20State%20ch%201-25%20-%20Joachim%20Hagopian.epub/
Thank you also, for writing your last book. I bought it, but still need to finish reading it. Although, I’ve already experienced all three aspects of the “mental health” industries’ systemic crimes, so probably none of it will be a surprise to me … however, it is very important information to be disseminated … so many thanks for writing it, Rob.
https://www.amazon.com/Your-Consent-Not-Required-Guardianships-ebook/dp/B09YR1RQLJ
Report comment
Rob i totaly agree with you’re point of view GREAT WORK KEEP GOING
Report comment
The mental health ‘experts’ have made expressing frustration, despair and hopelessness practically illegal.
Which is all that saying, “I wish my life were over” really means.
The ‘mental health’ system is run by idiots.
IMHO.
Report comment
Good cop: bad cop: sweat enough beneath him, touch him but you cannot reach him, see the sea, breath the air, inhale the breeze, from my surf, my waves from Jesus: don’t be a good cop, bad cop, and break up with the nature, soon to divorce her, imitate and prey on her, just to flee into the darkness of the night and we can’t trace you. It’s infinite blackness that echoes infinitely through itself to no-one. I am that pitch black, less then one. We are no-one. Bliss. Night.
Report comment